|
Case control studies are also known as "retrospective studies" and "case-referent studies." Teo, K. K. Ounpuu, S. Hawken, S. Pandey, M. Valentin, V. & Hunt, D. et al. (2006). Tobacco use and risk of myocardial infarction in 52 countries in the INTERHEART study: A case-control study. Lancet, 368(9536), 647-658. Each case is matched individually with a control according to certain characteristics such as age and gender. It is important to remember that the concordant pairs (pairs in which the case and control are either both exposed or both not exposed) tell us nothing about the risk of exposure separately for cases or controls. A patient who does not have the disease or outcome. Smedby, K. E. Hjalgrim, H. Askling, J. Chang, E. T. Gregersen, H. & Porwit-MacDonald, A. et al. (2006). Autoimmune and chronic inflammatory disorders and risk of non-hodgkin lymphoma by subtype. Journal of the National Cancer Institute, 98(1), 51-60. Care should be taken to avoid confounding a hero essay, which arises when an exposure and an outcome are both strongly associated with a third variable. Controls should be subjects who might have been cases in the study but are selected independent of the exposure. Cases and controls should also not be "over-matched." A case-control design offers an alternative that is much more efficient. The goal of a case-control study is the same as that of cohort studies, i.e. to estimate the magnitude of association between an exposure and an outcome. However, case-control studies employ a different sampling strategy that gives them greater efficiency. As with a cohort study, a case-control study attempts to identify all people who have developed the disease of interest in the defined population. This is not because they are inherently more important to estimating an association, but because they are almost always rarer than non-diseased individuals, and one of the requirements of accurate estimation of the association is that there are reasonable numbers of people in both the numerators (cases) and denominators (people or person-time) in the measures of disease frequency for both exposed and reference groups. However, because most of the denominator is made up of people who do not develop disease, the case-control design avoids the need to collect information on the entire population by selecting a sample of the underlying population. The odds of an event represent the ratio of the (probability that the event will occur) / (probability that the event will not occur). This could be expressed as follows: Question: Was the author correct in saying that the "odds" of a double-dip recession may have reached 50 percent? On Sept. 8 human resources case studies, 2011 the New York Times ran an article on the economy in which the writer began by saying "If history is a guide, the odds that the American economy is falling into a double-dip recession have risen sharply in recent weeks and may even have reached 50 percent." Further down in the article the author quoted the economist who had been interviewed for the story. What the economist had actually said was, "Whether we reach the technical definition [of a double-dip recession] I think is probably close to 50-50." The odds of disease in the exposed group are 7/10, and the odds of disease in the non-exposed group are 6/56. If I compute the odds ratio, I get (7/10) / (5/56) = 6.56, very close to the risk ratio that I computed from data for the entire population. We will consider odds ratios and case-control studies in much greater depth in a later module. However, for the time being the key things to remember are that: ', CAPTIONSIZE, 2, CGCOLOR, '#c00000', PADX, 5, 5, PADY, 5, 5,BUBBLECLOSE, STICKY, CLOSECLICK, CLOSETEXT how to critique a paper, ' ', BELOW, RIGHT, BORDER, 1, BGCOLOR, '#c00000', FGCOLOR, '#ffffff', WIDTH, 400, TEXTSIZE, 2, TEXTCOLOR, '#000000', CAPCOLOR, '#ffffff');">Rothman describes the case-control strategy as follows: Measurement of exposure can be made more comparable by using patients with other diseases as controls, especially if subjects are not told the exact focus of the investigation. However example thesis introduction paragraph, their exposures may be unrepresentative. To give an extreme example, a case-control study of bladder cancer and smoking could give quite erroneous findings if controls were taken from the chest clinic. If other patients are to be used as referents, it is safer to adopt a range of control diagnoses rather than a single disease group. In that way, if one of the control diseases happens to be related to a risk factor under study, the resultant bias is not too large. Sometimes interpretation is helped by having two sets of controls with different possible sources of bias. For example, a link has been suggested between the phenoxy herbicides 2,4-D and 2,4,5-T and soft tissue sarcoma. Some case-control studies to test this have taken referents from the general population, whereas others have used patients with other types of cancer. Studies using controls from the general population will tend to overestimate risk because of differential recall, whereas studies using patients with other types of cancers as controls will underestimate risk if phenoxy herbicides cause cancers other than soft tissue sarcoma. The true risk might therefore be expected to lie somewhere between estimates obtained with the two different designs. More chapters in Epidemiology for the uninitiated Usually it is not too difficult to obtain a suitable source of cases, but selecting controls tends to be more problematic. Ideally, controls would satisfy two requirements. Within the constraints of any matching criteria, their exposure to risk factors and confounders should be representative of that in the population "at risk" of becoming cases - that is, people who do not have the disease under investigation, but who would be included in the study as cases if they had. Also example of example essay topics, the exposures of controls should be measurable with similar accuracy to those of the cases. Often it proves impossible to satisfy both of these aims. Next time, an article will show how cross-tabulations are calculated, used, and interpreted in cohort and case-control studies. Case-control studies are relatively simple to conduct. They do not require a long follow-up period (as the disease has already developed), and are hence much cheaper. This design is especially useful for rare diseases (as you select the cases yourself), but not for rare causes (as you will probably not find these in sufficient number in your study). It is also very suitable for diseases with a long latent period, such as cancer. You select a group of children under five years free psychology case study examples, either all children of that age in the village, a random sample taken from the population register, or e.g. children living in the same area, or attending the same clinic. Then you classify them as either using the suspected water source or other water sources. You check e.g. after two weeks whether the children have had diarrhea. You can then calculate how many diarrhea cases there were among those children using the suspected water source and those using other sources of water supply (cumulative incidence of diarrhea). How to compare the cumulative incidence rates of the two groups, in order to conclude whether the suspected water source is a risk factor for the disease or not an opinion essay writing, will be discussed in a future blog. About the Author: With expertise in epidemiology, biostatistics and quantitative research projects, Annette Gerritsen, Ph.D. provides s ervices to her clients focussing on the methodological soundness of each phase of an epidemiological study to ensure getting valid answers to the proposed research questions. She is the founder of Epi Result .
Cohort studies work well for rare exposures –you can specifically select people exposed to a certain factor. But this design does not work for rare diseases –you would then need a large study group to find sufficient disease cases. Cohort studies begin with a group of people (a cohort) free of disease. The people in the cohort are grouped by whether or not they are exposed to a potential cause of disease. The whole cohort is followed over time to see if the development of new cases of the disease (or other outcome) differs between the groups with and without exposure. Notice the high study participation rate. Serum Carotenoids and Risk of Cervical Intraepithelial Neoplasia in Southwestern American Indian Women Come up with an answer to this question and then click on the icon to the left to reveal the answer. Control: Male 48 years of age (Person 47); Exposure status: Exposed There are two basic types of case-control studies, distinguished by the method used to select controls. The first is a non-matched case-control study in which we enroll controls without regard to the number or characteristics of the cases. In this study design, the number of controls does not necessarily equal the number of cases. For example, we may enroll 105 cases and 178 controls. Analytic methods for non-matched case-control studies include: The other basic type is a matchedcase-control study. In a matched study, we enroll controls based upon some characteristic(s) of the case. For example, we might match the sex of the control to the sex of the case. The idea in matching is to match upon a potential confounding variable in order to remove the confounding effect. (We will look at how matching occurs in the example below.) Can you think of more than one reason why a matched case-control study could take longer to complete than an unmatched study? How were cases and controls determined? Are the demographic characteristics similar for cases and controls? With case-control studies, we essentially work down the columns of the 2 × 2 table. Cases are identified first, then controls. The investigator then determines whether cases and controls were exposed or not exposed to the risk factor. We calculate the odds of exposure among cases (A/C) and the odds of exposure among controls (B/D). The odds ratio is then (A/C)/(B/D), which simplifies, after cross-multiplication, to (A*D)/(B*C). If this was a non-matched study check your english essay, the case would be counted in cell A in the preceding table because he is exposed. However, in the age- and gender-matched case-control study we must also find a male control within five years of age. Searching in the appropriate control population, we locate the following control: How do the results support the conclusions (Table 2 and conclusions)? The potential for selection bias in case control studies is a particular problem when cases and controls are recruited exclusively from hospital or clinics. Hospital patients tend to have different characteristics than the population, for example they may have higher levels of alcohol consumption or cigarette smoking. If these characteristics are related to the exposures under investigation, then estimates of the exposure among controls may be different from that in the reference population, which may result in a biased estimate of the association between exposure and disease. Berkesonian bias is a bias introduced in hospital based case-control studies, due to varying rates of hospital admissions. As the potential for selection bias is likely to be less of a problem in population based case-control studies, neighbourhood controls may be a preferable choice when using cases from a hospital or clinic setting. Alternatively, the potential for selection bias may be minimized by selecting controls from more than one source, such as by using both hospital and neighbourhood controls. Selection bias may also be introduced in case-control studies when exposed cases are more likely to be selected than unexposed cases. The procedures used for the collection of exposure data should be the same for cases and controls. Formulation of a clearly defined hypothesis Selection of cases The odds ratio (OR) is used in case-control studies to estimate the strength of the association between exposure and outcome. Note that it is not possible to estimate the incidence of disease from a case control study unless the study is population based and all cases in a defined population are obtained.
Measuring exposure status
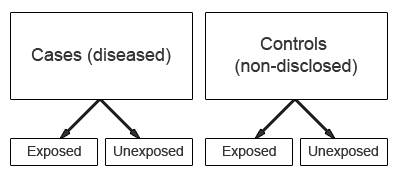
5. For information about Epi Info (Version 6), a word processing essay capital punishment against, database, and statistics program for epidemiology on microcomputers, please contact Centers for Disease Control and Prevention, Atlanta, GA 30333. [contact The Division of Surveillance & Epidemiology, Epidemiology Program Office] Matching controls to cases will mitigate the effects of confounders. A confounding variable is one which is associated with the exposure and is a cause of the outcome. If exposure to toxin ‘X’ is associated with melanoma, but exposure to toxin ‘X’ is also associated with exposure to sunlight (assuming that sunlight is a risk factor for melanoma) virginia polytechnic institute thesis, then sunlight is a potential confounder of the association between toxin ‘X’ and melanoma. In the analysis stage, calculate the frequency of each of the measured variables in each of the two groups. As a measure of the strength of the association between an exposure and the outcome, case-control studies yield the odds ratio. An odds ratio is the ratio of the odds of an exposure in the case group to the odds of an exposure in the control group. It is important to calculate a confidence interval for each odds ratio. A confidence interval that includes 1.0 means that the association between the exposure and outcome could have been found by chance alone and that the association is not statistically significant. An odds ratio without a confidence interval is not very meaningful. These calculations are usually made with computer programmes (e.g. Epi-Info). Case-control studies cannot provide any information about the incidence or prevalence of a disease because no measurements are made in a population based sample. Within what period of time after operation will the development of endophthalmitis qualify as a case – one day, one week, or one month? Will endophthalmitis have to be proven microbiologically, or will a clinical diagnosis be acceptable? Case-control studies may prove an association but they do not demonstrate causation. Consider a case-control study intended to establish an association between the use of traditional eye medicines (TEM) and corneal ulcers. TEM might cause corneal ulcers but it is also possible that the presence of a corneal ulcer leads some people to use TEM. The temporal relationship between the supposed cause and effect cannot be determined by a case-control study. A case-control study is designed to help determine if an exposure is associated with an outcome (i.e. disease or condition of interest). In theory, the case-control study can be described simply. First, identify the cases (a group known to have the outcome) and the controls (a group known to be free of the outcome). Then kinds of essay and its examples, look back in time to learn which subjects in each group had the exposure(s), comparing the frequency of the exposure in the case group to the control group. After clearly defining cases and controls, decide on data to be collected; the same data must be collected in the same way from both groups. Care must be taken to be objective in the search for past risk factors, especially since the outcome is already known, or the study may suffer from researcher bias. Although it may not always be possible, it is important to try to mask the outcome from the person who is collecting risk factor information or interviewing patients. Sometimes it will be necessary to interview patients about potential factors (such as history of smoking, diet, use of traditional eye medicines, etc.) in their past. It may be difficult for some people to recall all these details accurately. Furthermore, patients who have the outcome (cases) are likely to scrutinize the past, remembering details of negative exposures more clearly than controls. This is known as recall bias. Anything the researcher can do to minimize this type of bias will strengthen the study. Consider a situation in which a large number of cases of post-operative endophthalmitis have occurred in a few weeks. The case group would consist of all those patients at the hospital who developed post-operative endophthalmitis during a pre-defined period.
0 Kommentare
Hinterlasse eine Antwort. |

 RSS-Feed
RSS-Feed
